
-> Take Home Point vorweg : nach frühestens 8 Minuten.
Aber fangen wir von vorn an.
Ihr reanimiert primär erfolgreich eine/n Patient/in und schreibt so wie vorgesehen dieses EKG:
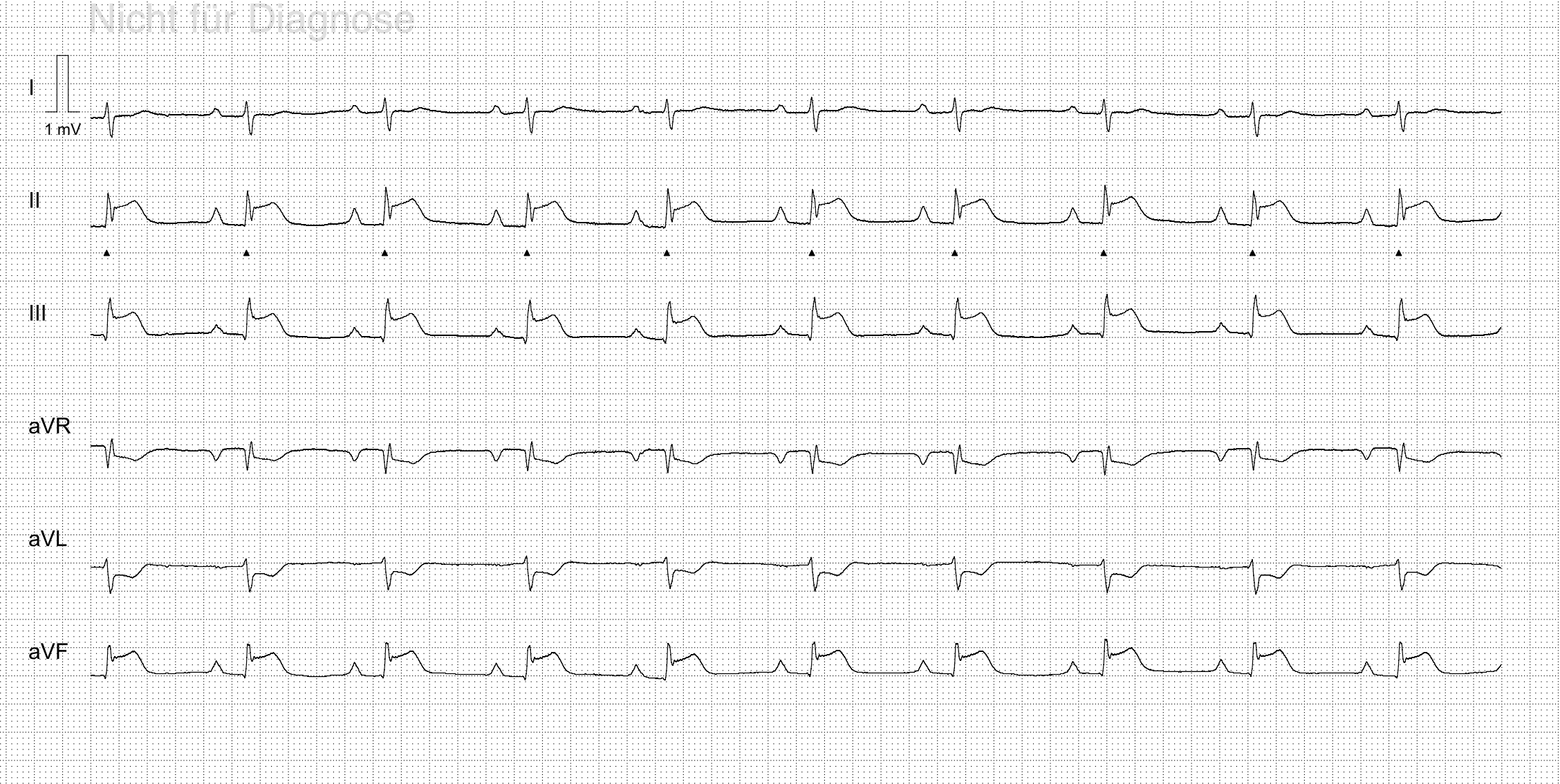
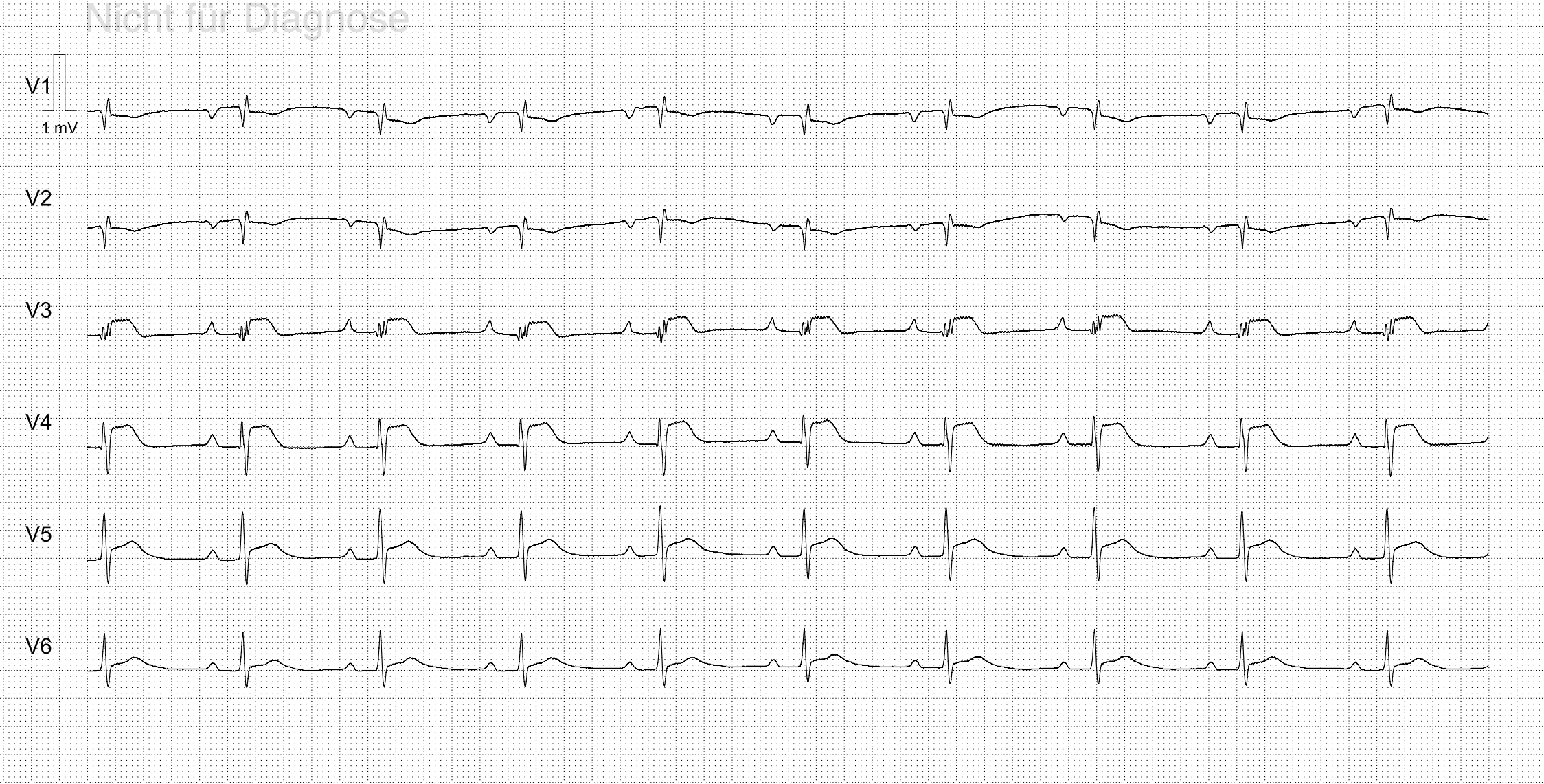
Ganz klar: Indikation zum Herzkatheter.
Jedoch…Ausschluss ACS- wie kann das sein?!
Kontext:
In ERC Kursen wird einem antrainiert, gleich nach ROSC das ABCDE-Schema abzuarbeiten.
Und wie wir alle wissen, gehört zu „C“ neben Blutdruck, Herzfrequenz etc. auch das EKG. Anhand dessen, entscheidet sich wohin wir unsere Patienten transferieren:
- OMI/very high risk NSTEMI in ein Herzkatheterlabor
- Alles andere kann warten. So wollen es die ESC Guidelines (5).
Unter stabilen Herz-Kreislaufverhältnissen.
Ein post-ROSC EKG ist jedoch alles andere als ein EKG unter stabilen Herz-Kreislaufverhältnissen. Was mit bis jetzt nicht bewusst war ist:
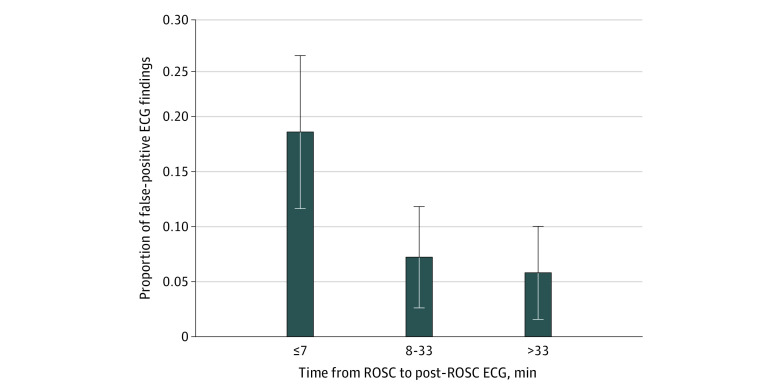
der optimale Zeitpunkt um ein EKG nach ROSC zu schreiben ist frühestens nach 8 Minuten (bzw. nach Restaurierung adäquater Perfusion):
„In cardiac arrest patients we have to deal with several issues, namely the global ischemia owed to the no-flow or the low-flow phase during cardiac arrest and the persistence of hemodynamic instability after ROSC, both of whom might decrease the diagnostic accuracy of standard ECG…
…These ischaemic electrocardiographic signs may disappear after restoration of good systemic perfusion as well as they may persist in case of persisting hypoperfusion….
…For all these reasons our suggestion is to abandon the old paradigm of acquiring the 12-lead ECG as soon as possible after ROSC rather at the right time and to implement the hemodynamic condition of the patients into the ECG interpretation.“
aus (4)
Es scheint so, dass innerhalb der ersten 7 Minuten nach HKS sich, aufgrund der stattgehabten Hypoperfusion, in etwa 20-30 % der Fälle eine ST-Hebung zeigt, welche sich im Herzkatheterlabor aber als nicht interventionspflichtige Läsion herausstellte. Somit ein falsch positiv gewertetes STE-ACS. (2, 3)
Somit wird diese scheinbar einfache Entscheidung doch ein wenig komplexer und aus einer Klasse I-B Empfehlung wird relativ schnell eine Klasse III-A Empfehlung:
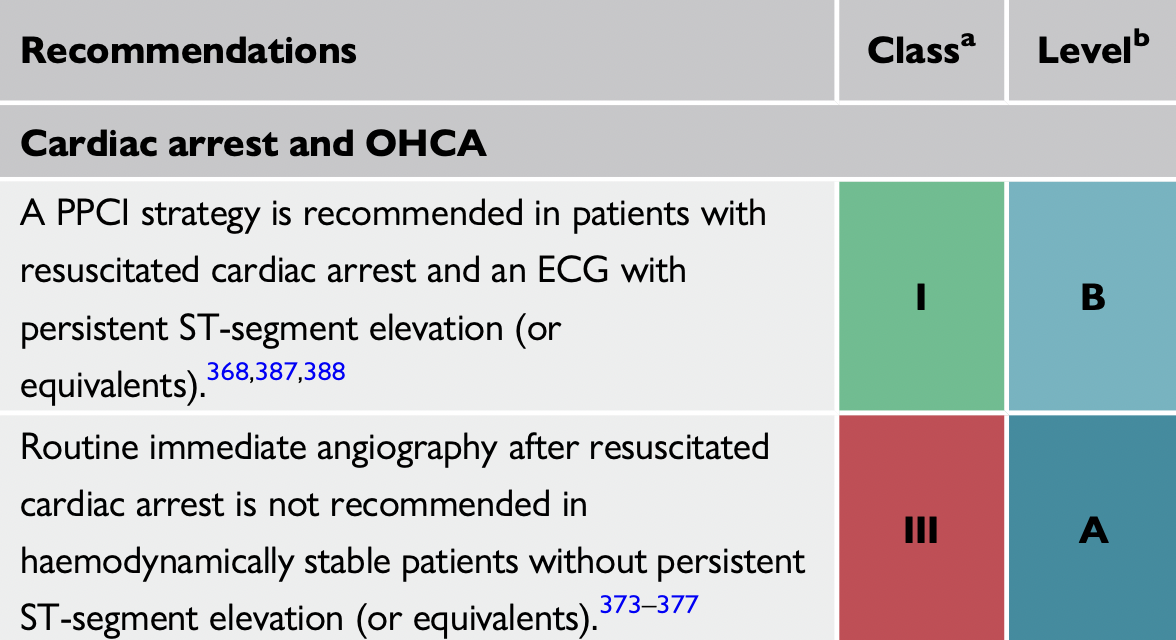
„We have, indeed, a class I indication for an immediate coronary angiography in case of a persistent ST-segment elevation and a very recent and appropriate class III indication for patients without a persistent ST-segment elevation…
… Few minutes can make the difference between a class I and a class III indication for an immediate invasive procedure.
(1)
Wir sollten anscheinend unsere Prioritäten nach ROSC ein wenig neu ordnen (auch wenn es gegen unseren bis dato trainierten Impuls widerstrebt) und das EKG-Schreiben hintanstellen. Meist ist es ja so, dass unmittelbar nach einem ROSC eh relativ viel auf einmal zu tun ist und wenn man diesen Punkt einfach ein wenig nach hinten (z.B. beim Einladen in den RTW/Hubschrauber) verlagert, sollte es zu keinem relevanten Zeitverlust kommen. Natürlich widerstrebt uns das, da es somit auch die Entscheidungsfindung verschiebt. Jedoch profitieren Patienten nur dann von einer Koronaragiographie, wenn auch wirklich eine Läsion zu intervenieren ist.
Literatur und Abbildungen:
- Savastano, Simone, Enrico Baldi, Sebastian Schnaubelt, and Angelo Auricchio. “Post Resuscitation ST-Segment Elevation: When a Few Minutes Make the Difference between a Class I and a Class III Indication for Immediate Coronary Angiography.” Resuscitation 192 (November 1, 2023): 109971. https://doi.org/10.1016/j.resuscitation.2023.109971.
- Baldi E, Schnaubelt S, Caputo ML, Klersy C, Clodi C, Bruno J, Compagnoni S, Benvenuti C, Domanovits H, Burkart R, Fracchia R, Primi R, Ruzicka G, Holzer M, Auricchio A, Savastano S. Association of Timing of Electrocardiogram Acquisition After Return of Spontaneous Circulation With Coronary Angiography Findings in Patients With Out-of-Hospital Cardiac Arrest. JAMA Netw Open. 2021 Jan 4;4(1):e2032875. doi: 10.1001/jamanetworkopen.2020.32875. PMID: 33427885; PMCID: PMC7801935.3
- Compagnoni S, Gentile FR, Baldi E, Contri E, Palo A, Primi R, Currao A, Bendotti S, Ziliani P, Ferrario Ormezzano M, Oltrona Visconti L, Savastano S. Peripheral perfusion index and diagnostic accuracy of the post-ROSC electrocardiogram in patients with medical out-of-hospital cardiac arrest. Resuscitation. 2021 Nov;168:19-26. doi: 10z.1016/j.resuscitation.2021.08.050. Epub 2021 Sep 8. PMID: 34506876.
- Alessandro Fasolino, Sara Compagnoni, Enrico Baldi, Guido Tavazzi, Johannes Grand, Costanza N.J. Colombo, Francesca Romana Gentile, Luca Vicini Scajola, Federico Quilico, Clara Lopiano, Roberto Primi, Sara Bendotti, Alessia Currao, Simone Savastano. Updates on Post-Resuscitation Care. After the Return of Spontaneous Circulation beyond the 2021 Guidelines. Rev. Cardiovasc. Med. 2022, 23(11), 373.
- 2023 ESC Guidelines for the management of acute coronary syndromes: Developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC)
- EMCrit.org Scott Weingart, MD FCCM. EMCrit RACC Lit Review – January 2024. EMCrit Blog. Published on January 23, 2024. Accessed on January 30th 2024. Available at [https://emcrit.org/emcrit/racc-lit-january-2024/ ].
- Amal Mattu ecgweekly.com October 30, 2022
